Clinical Information
Skull Base Surgery
Skull Base Tumor
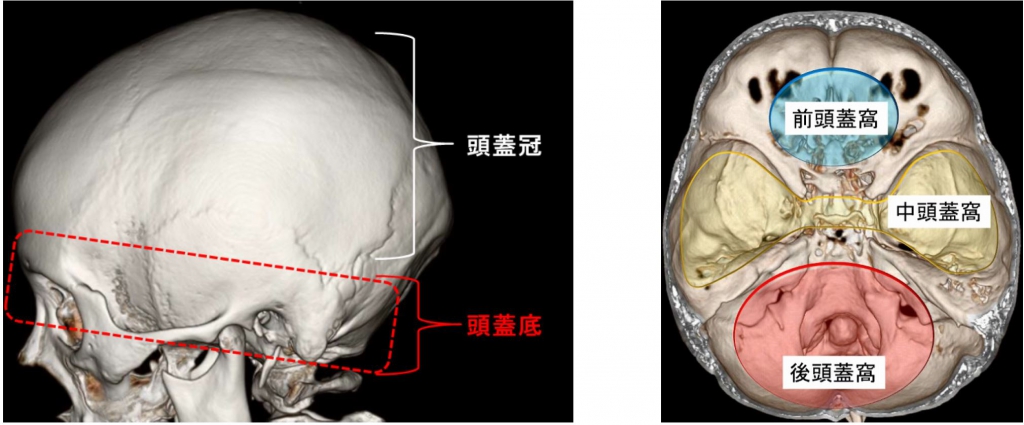
The base of the skull refers to the base of the skull and is classified into anterior, middle, and posterior cranial fossa, as shown in the figure below, and tumors arising from these areas are called skull base tumors. Skull base tumors are mainly benign tumors, such as meningiomas and schwannomas, with a high proportion of benign tumors. The base of the skull contains important structures such as the 12 cranial nerves, major intracranial arteries (such as the internal carotid and vertebral arteries) and the brain stem. Skull base tumors can grow to compress and engulf these structures. Hence, they are often found in cranial nerve symptoms and brainstem compression symptoms. The indication for treatment is comprehensively determined by the size of the tumor as well as the degree of brainstem compression and cranial nerve symptoms.
Our Treatment Guidelines
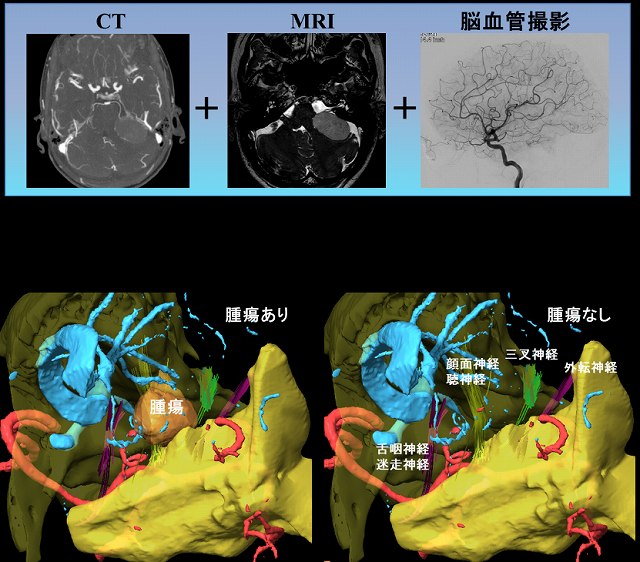
1) Surgical planning with 3-dimensional evaluation of the structures around the tumor
A 3D constructed image of the fused CT, MRI, and cerebral angiography images is created preoperatively, and the surgical plan is carefully discussed at the department’s conferences. During the operation, we use navigation to check the extent of removal to the maximum extent by comparing it with the actual surgical field.
2) Intraoperative nerve monitoring to preserve nerve function
During cranial base surgery, it is important that the important nerves and arteries present at the base of the skull are not damaged during the process of removing the tumor. In order to safely complete the surgery, our facility, in cooperation with the anesthesiologists and laboratory technicians, uses a number of case specific brain nerve stimulation monitoring (primarily facial, glossopharyngeal, vagus, parasympathetic, and hypoglossal nerves), auditory monitoring (auditory brainstem response), motor function monitoring, and visual function monitoring, depending on the case. We use monitoring.
In combination with 1) and 2), if it is difficult to dissect the tumor and critical structures (nerves, blood vessels, brainstem, etc.), we may deliberately leave a portion of the tumor in place, prioritizing the preservation of nerve function.
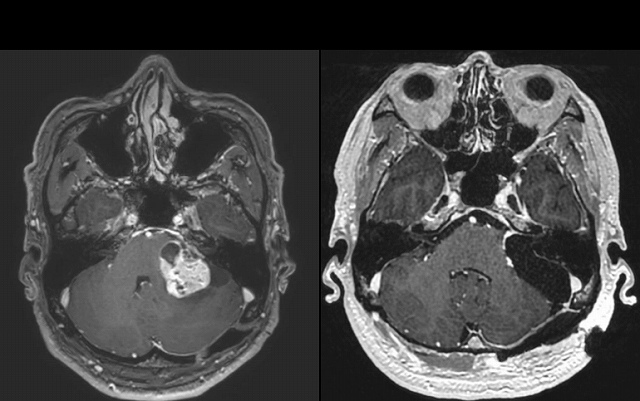
*In regard to auditory schwannoma and other pontine tumors
Since the tumor in this area compresses the facial nerve, we perform facial nerve stimulation during the operation to check the nerve.
In our hospital, in addition to facial nerve stimulation, continuous facial nerve monitoring is also performed during the tumor resection. By using this method, we believe it is possible to further reduce the risk of facial nerve damage.

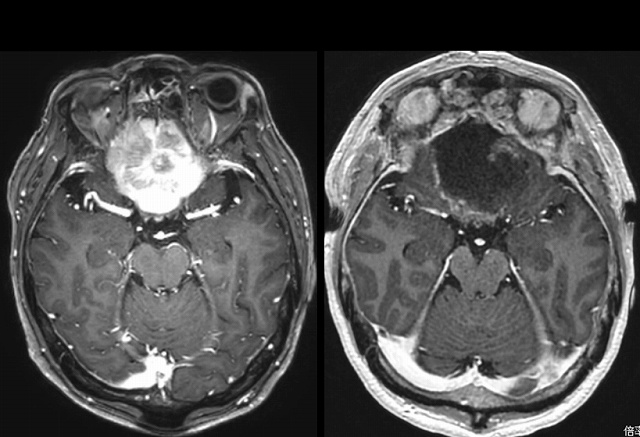
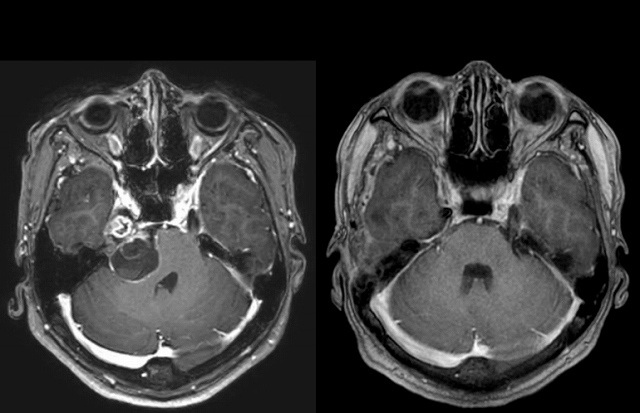
Representative cases